
- Cholesteatoma 101 - September 25, 2017
- Melanoma: Overview - September 25, 2017

- Risks of Surgery for Surfer’s Ear - October 26, 2017
- The Dangers of Untreated Exostosis / Surfer’s Ear - October 26, 2017
- Surfer’s Ear Treatment: Chisel vs Drill - October 26, 2017
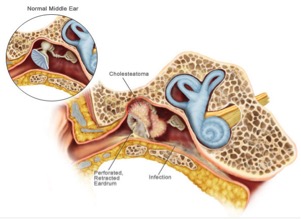
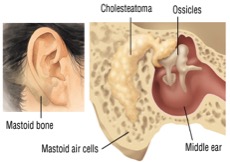
A cholesteatoma is the abnormal growth of skin in the middle ear. Although cholesteatoma is non-cancerous, the build-up of skin can act like a benign tumor by expanding and invading nearby structures. If not treated immediately, cholesteatomas may lead to permanent hearing loss, dizziness, facial muscle paralysis, and loss of taste.
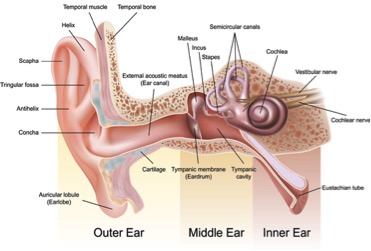
Basic Ear Anatomy
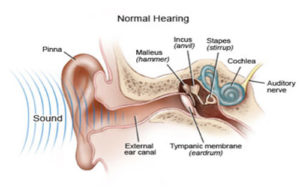
In order to understand cholesteatoma development, it is necessary to understand basic anatomy of the ear. The ear is separated in 3 sections: the outer ear, middle ear, and inner ear. The outer ear includes the helix and ear canal, the middle ear runs from the eardrum to the oval window, and the inner ear includes the cochlea and semicircular canals. Important structures include: tympanic membrane (eardrum), ossicles (three bones responsible for transmitting sound to the cochlea), eustachian tube (pressure equalization), cochlea (transforms sound into signals that are sent to the brain), and semicircular canals (send information on balance and position to the brain).
Cholesteatoma Classifications
There are three main ways in which a patient can develop a cholesteatoma:
- Congenital Cholesteatoma: The least common of classifications, congenital cholesteatoma begins during embryogenesis. Tissue attaches to the tympanic membrane with no history of ear infection, eardrum perforation, or ear surgery. The cause of congenital cholesteatoma is unknown.
- Primary acquired Cholesteatoma: Eustachian tube dysfunction, caused by chronic ear infections, sinus infections, colds, and allergies, are most associated with primary acquired cholesteatoma.
- Secondary acquired Cholesteatoma: Surgical trauma, acute ear infections, or general trauma to the middle ear can also lead to cholesteatoma. Trauma creates a perforated eardrum, or a hole, and allows skin into the inner ear.
The Eustachian Tube
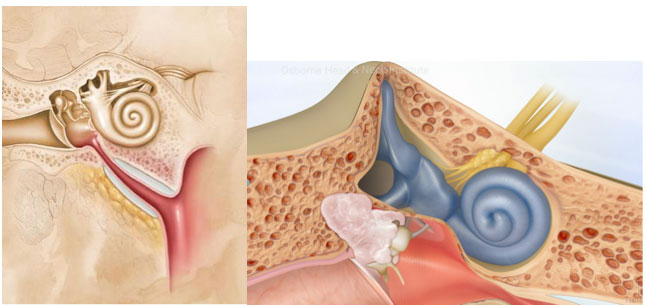
The eustachian tube is responsible for equalizing pressure in the middle ear. For this reason, when a person travels on a plane, climbs a mountain, or scuba dives, they can experience a “pop” in their ear. Connecting the middle ear to the nasopharynx (the back of the nasal cavity), the eustachian tube plays a vital role in maintaining a balanced environment for the ear. When blocked, air cannot flow in or out of the middle ear, creating negative pressure. Like a vacuum, negative pressure results in skin invagination. Skin, cells, fluids, and waste accumulate inside the middle ear. Furthermore, the ear depends on the eustachian tube for drainage; therefore, stagnant masses in the middle ear can lead to infection.
Symptoms of Cholesteatoma
Cholesteatoma growth and its effects develop over time. The longer one waits for treatment, the more serious that symptoms can become. It is advisable to seek prompt evaluation from an otologist, a hearing and balance specialist, at the first signs of cholesteatoma symptoms.
Early signs:
- Hearing loss in the affected ear
- Ear drainage (with or without odor)
- Ear Pressure
- Ear Pain
- Recurrent infections
Later signs:
- Dizziness/Imbalance
- Facial weakness
- Tinnitus (ringing in the ear)
- Taste Disturbance
Cholesteatoma can have negative long term effects. In the inner ear, nerves responsible for facial movement, taste, hearing, and balance are at risk when there is disruption of the skin. Long term effects can be prevented the sooner one seeks professional care.
Possible Long-Term Effects:
- Permanent Hearing Loss
- Facial Muscle Paralysis
- Meningitis
- Vertigo
- Ear Abscess aka Mastoiditis
Diagnosing Cholesteatoma
Initial signs of cholesteatoma can be identified with a thorough physical exam. In order to determine an exact diagnosis, the following tests may be performed:
- Audiograms and Tuning Forks: Hearing tests can determine the degree and type of hearing loss. While conductive hearing loss affects the outer and middle ear, sensorineural hearing loss affects in the inner ear. Tuning forks are another form of hearing tests; through the Weber and Rinne tests, an otologist can determine the type of hearing loss and damage that cholesteatoma may have caused.
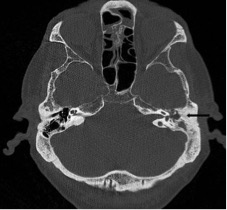
- Computed Tomography (CT): CT scans can identify mass density and spread. In a CT scan, black is air and opaque white is bone. The spectrum between is tissue or fluid. Cholesteatoma Is the same density as skin. If fluid is found in the middle ear, cholesteatoma would not be the final diagnosis.
- Magnetic Resonance Imaging (MRI): For more advanced cases, MRI scans may be necessary to rule out brain involvement. Cholesteatoma grows and can reach the cerebral membrane through the mastoid bone. MRI scans should be taken once cholesteatoma has been diagnosed to identify affected structures.
While physical exams may identify some aspects of cholesteatoma, imaging can confirm keratin growth. Tympanosclerosis, cholesterol granuloma, cerumen impaction, and abscess are other ear conditions that would otherwise be mistaken for cholesteatoma unless imaging was available.
Treatment and Reconstruction
To reiterate, cholesteatoma symptoms worsen with time. Due to it’s location, a cholesteatoma can spread into the inner ear or the brain. Growth cannot be stopped unless removed surgically. Cholesteatoma cases vary and some patients may need either one or all of the following procedures:
- Tympanoplasty: Most cases require the reconstruction of the eardrum through the use of skin grafts (from the back of the ear, tragus, or vein).
- Mastoidectomy: If skin is allowed to grow further into the mastoid bone (behind the temporal bone), a mastoidectomy is necessary to remove diseased mastoid air cells, which can lead to ear infection.
- Ossicular Chain Reconstruction: The ossicles are located near the tympanic membrane. Due to the location of most cholesteatomas, skin masses are very likely to spread to the middle ear and break the three bones (hammer, anvil and stirrup). Use of prosthesis or reconstructed hearing bones can restore ossicular vibration.
Cholesteatoma is the abnormal growth of keratin in the middle ear. Although cholesteatomas are not classified as either tumors or cancers, they can cause significant problems because of their erosive properties. Some of these issues include ossicular destruction, spread through the mastoid bone, and invasion into the brain. Cholesteatomas are often infected and can result in chronically draining ears. Any sign of cholesteatoma should be promptly evaluated by a specialist. Long periods of time may only worsen the condition and its possible long term effects.
For more information on otology and restorative hearing surgery, visit: www.eardoctorla.com

{kind=link}